Every time we experience something new, we are in the position of learning and memorising the new experience. Learning depends on several factors, including motivation, rewards, self-reflection, saliency, and repetition. One additional important aspect that seems crucial for learning is the presence of a prediction error. Accumulating evidence suggests that our brain is a predictive organ, holding prior internal representations of reality. The brain creates predictions based on its internal representation and tests the accuracy of such internal models with the sensory information coming from the external world (our body included) (Holland & Schiffino 2016). Put simply, if the external information matches with what is expected, everything goes on automatic pilot, with minimal energy expenditure. On the contrary, if the incoming information does not reflect the prediction (that is, there is a prediction error), then action needs to be taken in order to minimise the error. One way to deal with it is to update the prediction. The model updating is, effectively, learning.
In other words, it is easier to learn something that is surprisingly different from what we expect. That information will be efficiently stored in your neurons and is easier to retrieve. That is, it acquires storage strength. Storage strength also depends on how long ago the information was stored, how frequently you (need to) retrieve it, and how relevant is that information. In the case of a potentially fatal, aversive situation, the experience holds high intrinsic relevance and will thus be hard-wired in your neurons. If you are about to drink some milk from the bottle and at the first sip you realise that you have just drunk bleach; that unexpected and potentially fatal experience will be remembered for a very long time. It is very likely that you will start smelling the milk before drinking it from that moment on.
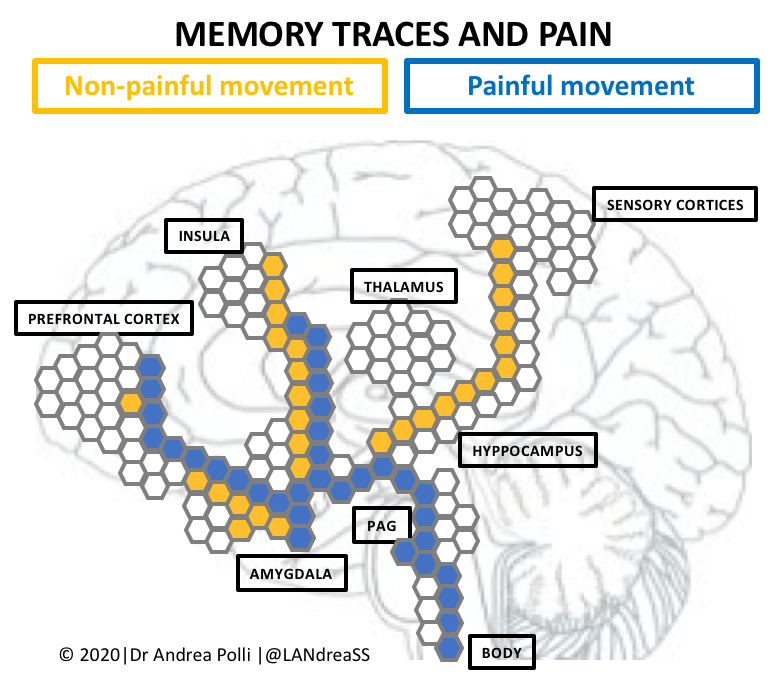
The same can be said for pain.
Pain holds an innate aversive connotation. It informs us of potential damage, injury, or lesions; and it is normally interpreted as such. From an evolutionary viewpoint, it is important for survival to give pain full consideration. Once one movement or activity becomes painful, it quickly catches our attention; the nervous system learns the association and the more the relevance that movement has for us, the more that memory trace gains storage strength. If your left middle finger starts to hurt, it will be more important if you are a professional pianist, getting closer and closer to the next important concert, than if you are, say, a right-handed school teacher.
At this point, the treatment approach seems logical. We need to find a way to erase the memory trace encoding the learnt association between movement and pain and promote the pain-free one (Zusman 2008; Nijs et al. 2014) – the so-called inhibitory learning. However, this is complicated by what we know about memory and how it is stored. Memories cannot be erased. Inhibitory learning is actually new learning, creating a new memory trace.
This has clear clinical implications.
Let’s assume we can easily create a new memory encoding for painless, fearless, movement (which it isn’t easy at all for a start!). We are now left with two traces that will be competing with one another. Only one of the two will be activated. Importantly, activation is unconscious and depends, again, on storage strength. As mentioned, given the very nature of pain and its relevance for survival, pain memories are hard-wired and will likely be prioritised in the process. Which means that clinicians need to work extra hard to maximise the storage-strength of the new memory and make it more retrievable.
Here is where expectancy violation can come in hand. As the name suggests, this paradigm aims to violate the (negative) expectations that patients have about their pain. From the brain perspective, expectancy violation is a way to create a prediction error. Maximising the prediction error is thus one way to strengthen the inhibitory learning. Most research on inhibitory learning is conducted in the field of psychology, where expectancy violation is used as a principle to design exposure therapy in the treatment of phobias and anxiety. Unfortunately, about 40-50% of the patients undergoing an exposure therapy do not show significant improvements. For instance, patients with mental disorders or trait anxiety tend to show non-significant changes after the treatment. In some cases, expectations are not changed even after a successful violation. It is not uncommon for patients to attribute the reason of the violation to contextual factors. In fact, expectancy violation seems to be highly context-specific (Craske et al. 2018).
Can we transfer all this to the pain field?
Exposure therapy has been proposed for the treatment of chronic pain as well (Meulders 2020). Some studies show promising results. However, when exposure-based treatments are compared to graded activity or graded exercise (which do not explicitly target feared activities or movements) exposure therapy seems effective in reducing negative emotions associated with pain, but not pain itself or disability (George et al. 2010). At least no more effective than the control treatments. This partially questions the relevance of the expectancy violation paradigm to treat pain, and suggests that other aspect might be more relevant for improving pain and reducing disability, such as motivation and self-efficacy.
Another aspect to consider might be that exposure therapies, as proposed in chronic pain, do not really maximise expectancy violation. To the best of my knowledge, protocols include a preliminary part focussed on explaining to the patient that pain does not equal damage or injury, thus de-threatening it (Vlaeyen et al. 2002). Furthermore, exposure commonly starts from activities that are little or mildly feared, to then proceed to the next one once the previous one is successfully treated. For what I can understand, this would actually minimise the prediction error and consequently inhibitory learning. Is it possible that by educating the patient about the non-always-threatening nature of pain, we actually make exposure therapy less effective? We seem to find ourselves in the paradoxical situation in which education hinders learning.
It would be very interesting to see treatments that are actually designed to maximise expectancy violation. To do so, we can again try to steal the principles from the treatment of phobias. Michelle Craske suggests a number of strategies such as making negative expectations as precise and explicit as possible in order for them to be clearly violated, lengthen the time between sessions, remove safety strategies, and make use of so-called deepen extinction in order to help generalisation of the new learning (Craske et al. 2014). In addition, we it might be helpful to avoid patient’s education in the early stage of the treatment, and perhaps post-pone it to after expectations have been violated and use it more as a sort of self-reflection. I don’t know if this would be the definitive answer to treating chronic pain – I honestly doubt it – but my guess would be that a real maximisation of expectancy violation would help achieve the same results of the currently used exposure therapies, but in less time.
In any case, it seems like an exciting avenue to undertake.
Andrea POLLI
Andrea Polli is a physiotherapist and OMT manual therapist. After his master in rehabilitation of musculoskeletal disorders and a few years in clinical practice, he moved from Italy to the UK, to obtain the MSc in Pain: Science & Society at the prestigious King’s College London. He then returned to Italy for a few years, working as a physiotherapist at the IRCCS San Camillo Hospital, in Venice. He is part of the Pain in Motion group since 2015, based at the Vrije Universiteit Brussel and KU Leuven. In 2020, he obtained his PhD working on a project that explored whether epigenetic changes can play a role in helping people with persistent pain.
2020 Pain in Motion
References and further reading:
Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B. Maximizing exposure therapy: an inhibitory learning approach. Behav Res Ther. 2014 Jul; 58:10-23. doi: 10.1016/j.brat.2014.04.006.
Craske MG, Hermans D, Vervliet B. State-of-the-art and future directions for extinction as a translational model for fear and anxiety. Philos Trans R Soc Lond B Biol Sci. 2018 Mar 19;373(1742):20170025. doi: 10.1098/rstb.2017.0025.
George SZ, Wittmer VT, Fillingim RB, Robinson ME. Comparison of graded exercise and graded exposure clinical outcomes for patients with chronic low back pain. J Orthop Sports Phys Ther. 2010 Nov;40(11):694-704. doi: 10.2519/jospt.2010.3396.
Holland PC, Schiffino FL. Mini-review: Prediction errors, attention and associative learning. Neurobiol Learn Mem. 2016 May; 131:207-15. doi: 10.1016/j.nlm.2016.02.014.
Meulders A. Fear in the context of pain: Lessons learned from 100 years of fear conditioning research. Behav Res Ther. 2020 Aug; 131:103635. doi: 10.1016/j.brat.2020.103635
Nijs J, Lluch Girbés E, Lundberg M, Malfliet A, Sterling M. Exercise therapy for chronic musculoskeletal pain: Innovation by altering pain memories. Man Ther. 2015 Feb;20(1):216-20. doi: 10.1016/j.math.2014.07.004.
Vlaeyen JW, de Jong J, Geilen M, Heuts PH, van Breukelen G. The treatment of fear of movement/(re)injury in chronic low back pain: further evidence on the effectiveness of exposure in vivo. Clin J Pain. 2002 Jul-Aug;18(4):251-61. doi: 10.1097/00002508-200207000-00006.
Zusman M. Associative memory for movement-evoked chronic back pain and its extinction with musculoskeletal physiotherapy. Phys Ther Rev, 2008, 13.1: 57-68. doi: doi.org/10.1179/174328808X251948
{kind=link}