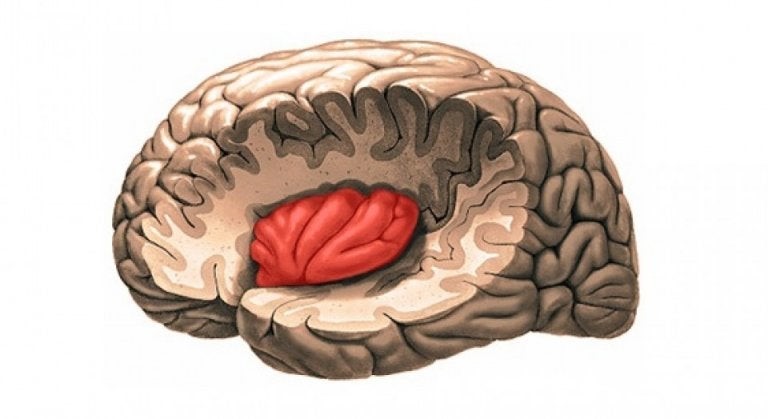
In Europe, 1 in 5 people suffer from chronic pain, which means that we all know someone who is struggling with chronic pain complaints. This pain can be located in a specific region, such as migraine or chronic low back pain, but can also occur all over the body as is the case in fibromyalgia. Fibromyalgia occurs in 1 in 20 people and is characterized by chronic widespread muscle aches and muscle stiffness, but when we study the muscles histologically we see no damage or degeneration of the muscles. So there are no muscle abnormalities that can explain the muscle aches, and consequently we need to start looking for the cause in the central nervous system where the pain signals are processed. The processing of pain in the central nervous system is affected by autonomic and neuro-endocrine processes. The insula is one of the most important brain regions involved in the processing of pain, and does not only process sensory information about pain stimuli (pinpoint the location of the stimuli, determining the type of stimuli, how threatening the stimuli ate, etc.) but is also determining how we respond to pain stimuli (what we think, how we will adjust our behaviour). It has previously been shown that with increased pain sensitivity, as is the case in fibromyalgia, the insula will adapt functionally and anatomically.
But in addition to the muscle pain complaints, fibromyalgia patients also experience many other complaints throughout the body. This makes it difficult to identify one specific underlying mechanism, and because currently there is no general consensus on the underlying mechanism, fibromyalgia patients often feel misunderstood and are not adequately treated. This has motivated us to put together a multidisciplinary team with relevant expertise and with this team we recently put forward a new hypothesis regarding the mechanism of fibromyalgia and published it in the international scientific journal Medical Hypotheses. We postulate that a specific brain region, in particular the insula, plays a key role in the chronic symptoms experienced by fibromyalgia patients. More specifically, by bringing together findings from several existing studies and looking at the bigger picture, we were able to conclude that within the insular cortex the balance between the excitatory neurotransmitter glutamate (Glu) and the inhibitory transmitter gamma-amino butyric acid (GABA) is disturbed. This provides an explanation not only for the experienced muscle pain that these patients experience, but also for the various other symptoms they experience such as dysregulation of heart rate and blood pressure, bladder and bowel symptoms, sleep disturbances, chronic fatigue, and autonomic dysfunction to name a few.
If we delve deeper into this neurotransmitter imbalance, which are signal or messenger substances in our body, then the neurotransmitter glutamate plays an important role. This neurotransmitter causes a sensitization or hypersensitivity of the central nervous system, and we see that levels of this glutamate together with glutamine (a precursor to the synthesis of Glu or GABA) within the insula are higher in fibromyalgia patients compared to healthy people, and that this is associated with higher pain sensitivity (e.g. lower pain thresholds). Not only is there a molecular imbalance in the insula of fibromyalgia patients, but MRI research also shows changes in brain activity and connectivity.
The insula is responsible for regulating heart rate and blood pressure. In fibromyalgia patients, cardiovascular symptoms such as irregular heartbeat, decreased heart rate variability, orthostatic intolerance (postural tachycardia syndrome), autonomic dysfunction, etc. are known problems. The insula is also involved in the processing of signals from the bladder, bringing a full bladder to our conscious attention to motivate appropriate bladder emptying. Fibromyalgia patients often suffer from bladder dysfunctions. Glutamate is involved in the regulation of brain-gut communication, through the so-called brain-gut axis. The neurotransmitter conveys information to and from the gut to the brain, sending signals to appropriately control gut secretion and motility. Inappropriate control of this system can lead to irritable bowel syndrome, a condition which is frequently established in fibromyalgia. Unrefreshing sleep, poor sleep quality, obstructive sleep apnoea and fatigue are also common reported symptoms and may be caused by autonomic dysfunction or changes in the brain linked to the insula. Psychiatric comorbidities, such as anxiety and mood disorders, are common in chronic pain conditions like fibromyalgia and accumulating evidence shows altered insular activation in individuals with dysregulated mood or anxiety. Small fibre pathology refers to damage to the small unmyelinated peripheral nerve fibres that run through our skin, peripheral nerves and organs and occurs very frequently in fibromyalgia. Typically a reduction of the intra-epidermal nerve fibre density is observed, which can lead to pain, tingling, sensory disturbances, etc. This could be a consequence of a functional reorganization of the peripheral nervous system in response to hyperactivity of the central nervous system. Animal studies have shown that elevated levels of insular glutamate will lead to a reduction in intra-epidermal nerve fibre density contributing to small fibre pathology. And by manipulating the levels of this neurotransmitter in rats, these rats showed fibromyalgia-like symptoms, suggesting that the presence of small fibre pathology, increased release of glutamate at the brain and fibromyalgia related symptoms are linked to each other.
The good news is we are now making progress by better understanding the disease mechanisms of fibromyalgia. With regard to diagnosis, patients used to rely on an exclusion approach, whereas at present a first 'positive' test is available with the detection of small fibre pathology. Through specific brain imaging, we can detect changes in neurotransmitter (glutamate or gamma-aminobutyric acid) balance in the brain. The new mechanistic insights also lead to the development of new treatment strategies for fibromyalgia. Pharmacological treatment is now aimed at influencing the sensitivity of receptors to which glutamate binds and thus controlling the concentration of released glutamate. The receptors work too well in fibromyalgia, which results in too high concentrations of glutamate in the body and which we want to counteract. There is experience with drugs such as ketamine that act on increased glutamate receptor activity and lead to pain relief, however these types of medication can also induce adverse side effects. Several new pharmacological neuromodulators are currently being tested, and initial results of early test studies are promising. The use of brain stimulation techniques (such as (non)invasive rTMS and tDCS, and invasive deep brain stimulation) is also further explored as a way to normalize brain function. But it has also been shown that regular physical activity can lead to restoration of hyper connectivity between brain regions (including the insula) and prevent the hypersensitivity of glutamate receptors. Furthermore, solid evidence is available for the beneficial effect of physical activity (especially aerobic exercise and strength training) on fibromyalgia symptoms.
Jessica Van Oosterwijck
Jessica Van Oosterwijck is an Associate Professor in the field of chronic disorders and pain at Ghent University (Belgium), which she combines with a post-doctoral research fellowship funded by the Research Foundation - Flanders (FWO). She is also a Visiting Professor at the Department of Rehabilitation Sciences and Physiotherapy of the University of Antwerp (Belgium), and a founding member of the Pain In Motion international research group.
2020 Pain in Motion
Reference for further reading:
Boel De Paepe, Joél Smet, Chris Baeken, Jessica Van Oosterwijck, Mira Meeus. A capital role for the brain’s insula in the diverse fibromyalgia-associated symptoms. Medical Hypotheses 2020;143:110077
https://doi.org/10.1016/j.mehy.2020.110077
https://www.sciencedirect.com/science/article/abs/pii/S0306987720309361#!
{kind=link}