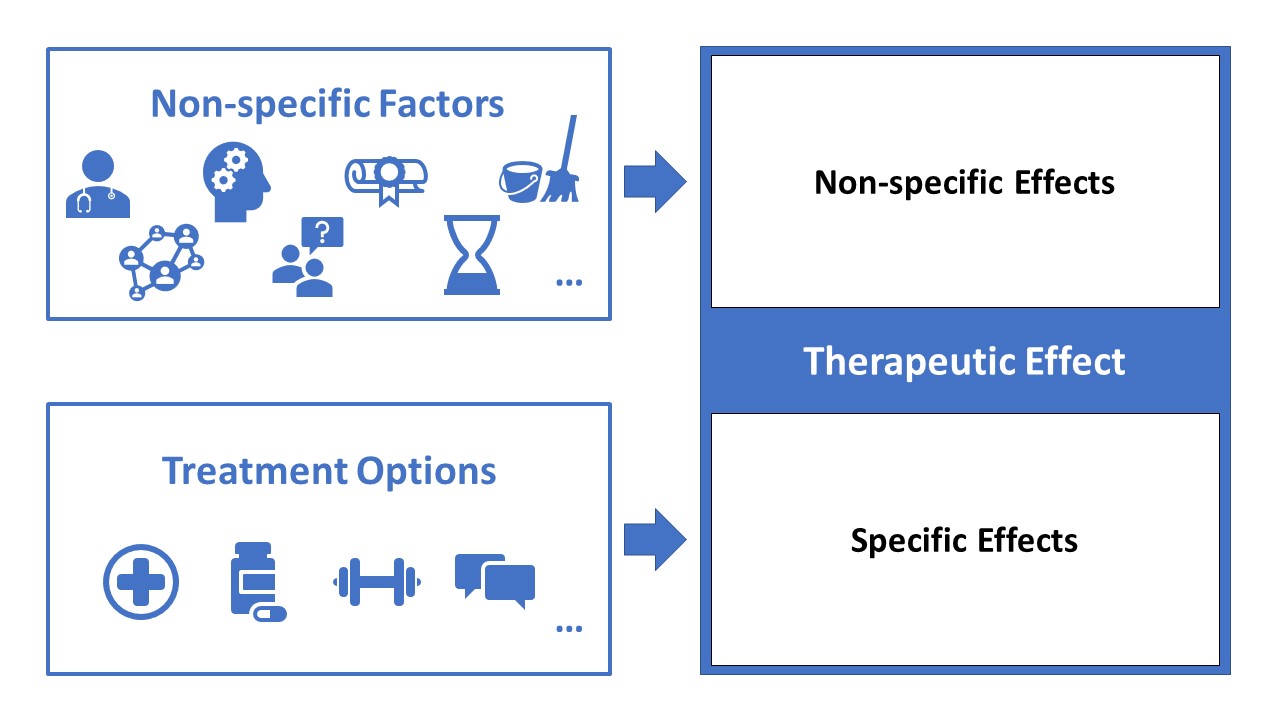
Did you ever wonder why a specific treatment does not always have the same effect in one person compared to another despite having the same problem? When using painkillers for example, some people experience almost immediate pain relief while others (with the same complaints) seem to benefit less from the same dose. A lot of differences in treatment results can be explained by contextual factors and non-specific treatment effects. The final result of a treatment (in this case pain relief) can be explained on the basis of both the specific and non-specific treatment effects and is also referred to as the therapeutic effect.
Specific treatment effects are treatment effects that can be explained by the treatment itself, namely the effect that is unique and "specific" for this treatment. Non-specific treatment effects are the effects of factors and interactions that are not specific to the treatment itself. You probably immediately think of the placebo effect. Indeed, the placebo effect is a non-specific positive effect that is observed when using a placebo treatment (e.g. administering a non-active substance as a painkiller). The counterpart of this is the nocebo effect or a perceived adverse effect from an intervention. I also want to address a common misconception about the placebo effect. Sometimes you hear people say: “a placebo effect is not a real effect, it is something in your head”, indicating that a placebo is only something psychological. Although this seems plausible, there is compelling evidence that indicates that placebo interventions can lead to neurophysiological changes which in the end benefit the treatment outcomes (Testa, 2016; Benedetti, 2016a; Benedetti, 2016b; Benedetti, 2013).
Non-specific treatment factors influencing the treatment outcome will always be present. In general we can split these up in five groups: the patient, the clinician, the therapeutic alliance, treatment related factors, and the environment. I will describe some of these factors in these categories so you can get an idea.
The patient
One of the most important factors is the expectation of a patient. Patients’ expectations shape their pain experience and can greatly influence the general treatment outcome. Most of the time, the influence of expectations is underestimated and rarely addressed by clinicians (Barron, 2007; Bialosky, 2010; Puentedura, 2012). Prior experiences of the patient such as similar treatments, prior contact with the clinician, stories of other people can greatly affect their expectations and preferences, and therefore affect the outcome of the therapy (Colloca, 2006; O'Keeffe, 2015). Expectations are closely related to illness perceptions, which are getting more attention in treatment nowadays. Addressing wrong illness perceptions and cognitions during the assessment and treatment can help to tackle wrong expectations and improve treatment outcome (Petrie 2019). Several studies also showed that there are gender and age differences in treatment satisfaction despite receiving the treatment in the same setting (Stenberg et al., 2012, hush et al. 2011). We also have to consider natural history of the patient: without any treatment our patient would (in most cases) improve over time due to a natural healing process.
The clinician
The way a clinician looks and his reputation in general have an impact on the treatment outcome. It is the patients’ perceptions about the professionalism, expertise ,and reputation of the clinician that are important factors that can contribute to a positive clinical outcome (Testa et al. 2016). Furthermore, the way a clinician behaves during the consultation and treatment seems to modify the outcome too. Optimistic and confident clinicians who take the time to listen to their patient, encourage questions, deliver positive feedback, and give clear information about the condition and treatment seems to get better results (Lucassen, 2016; Testa, 2016). Contrary, clinicians who are nervous, use difficult medical jargon, are in a hurry, and spend too much time reading patients charts are negatively impacting the treatment outcome (Testa, 2016). Beliefs of the clinicians about the probable outcome impact the outcome itself too (Testa, 2016). Positive beliefs result in an improvement while negative beliefs results in worsening of the outcome (Sternberg, 2011). For example, the study by Gracely et al. indicates that the beliefs of the person delivering the treatment (in this case dentists) have the potential to change the pain production of the brain. In this particular study, dentists were asked to deliver an active drug to reduce pain in one group and a placebo in another group. However, both groups received a placebo without the knowledge of the dentists and patients. Results showed an increase of pain in the second group (of whom the dentist thought they received a placebo) and a decrease in pain in the first group (of whom the dentist thought they received an active drug) after the intervention (Gracely, 1983). This shows that that the beliefs of the person delivering the treatment can influence the outcome. The results also indicate that patients are able to unconsciously pick up cues from the clinician, influencing the pain mechanism of the patient.
The therapeutic alliance
The therapeutic alliance refers to the relation, a sense of collaboration and support, between the patient and the clinician. Several studies in physical, cardiac, and neurological rehabilitation have shown that positive alliances are associated with better treatment outcomes (Ferreira, 2013; Schönberger M,2007; Burns, 2007; Flückiger C, 2018). A recent study of Brunner et al. reports that higher self-reported confidence in managing the patient by physiotherapists was associated with higher patient-reported alliance measured (Brunner, 2019). Furthermore, positive verbal and non-verbal communication seem to positively influence the therapeutic alliance (Testa et al. 2016).
Treatment related factors.
Besides the effect of the treatment itself (specific treatment effect) there are some related factors such as the way the treatment is delivered by the clinician. A personalized treatment considering the patient’s opinions benefits the treatment outcome. Moreover, a clear explanation about the diagnoses and the (possible) treatment, delivering all treatment sessions by the same clinician, punctuality, flexibility, and an adequate treatment duration and follow-up positively affect the satisfaction of the patient. Furthermore, if patients can watch and talk to other patients that successfully received a similar treatment, a better treatment outcome can be expected (Colloca, 2014). A study of Branthwaite and Cooper showed that branded analgesic and a branded placebo were more effective in relieving pain than their non-branded variant respectively (Branthwaite, 1981). So the branding of medication/placebo on his own has an effect. There are also some treatment related factors that negatively influence the treatment outcome (e.g. lack of privacy, waiting list, expensiveness, hastened treatment) (Testa 2016).
Environment
The patient’s outcome can be modulated by several factors of the environment such as lightening, relaxing sound, cleanliness, adequate temperature, accessibility, and supporting staff (Testa et al. 2016, Hush et al., 2011). In general, when the patient does not experience the environment as unpleasant, a positive influence on the treatment can be expected.
There are a lot of contextual factors that can influence the therapeutic effect of a treatment due to nonspecific treatment effects. As a clinician or researcher, it can be difficult to control all these non-specific factors, especially since all influencing factors are not known yet. However, researchers should try to minimalize differences in the non-specific treatments effects between the different treatment groups so that the difference found between these groups is a real representation of the difference in a specific treatment effect. In my opinion, every clinician should aspire the largest possible therapeutic effect by choosing the right treatment (i.e. treatment with a sufficient specific effect), taking contextual factors into account, and making sure they are doing more than a placebo treatment.
What do you think about contextual factors and their non-specific treatment effects? Do you think we should use these effects?
Delivering a treatment that works is the most important part. Whether the effect is specific or non-specific does not matter.
Always treat patients with the right treatment (i.e. treatment with a large specific effect). Non-specific effects are not that important.
Choosing a treatment that fits the patient by taking contextual factors and potential non-specific effects into account, and which is effective for their problem (i.e. treatment with a sufficient specific effect) is preferable.
Contextual factors and non-specific effects make or break your treatment. These should be prioritized in the treatment decision.
Other opinion.
You can answer by clicking on this link: https://linkto.run/p/R52VOL84
The results can be followed by clicking the following link: https://linkto.run/r/R52VOL84
Thomas Bilterys
Thomas Bilterys is a doctoral researcher at the Vrije Universiteit Brussel (Brussels, Belgium) and Ghent university (Ghent, Belgium). His research and clinical interest goes out to chronic pain and associated sleep problems.
2019 Pain In Motion
References and further reading:
Testa M, Rossettini G. Enhance placebo, avoid nocebo: How contextual factors affect physiotherapy outcomes. Man Ther. 2016 Aug;24:65-74. doi: 10.1016/j.math.2016.04.006. PubMed PMID: 27133031
Benedetti F, Frisaldi E, Carlino E, et al. Teaching neurons to respond to placebos. J Physiol 2016;594:5647–60. PubMed PMID: 26861164
Benedetti F, Carlino E, Piedimonte A. Increasing uncertainty in CNS clinical trials: the role of placebo, nocebo, and Hawthorne effects. Lancet Neurol 2016;15:736–47. PubMed PMID : 27106073
Benedetti F, Thoen W, Blanchard C, et al. Pain as a reward: changing the meaning of pain from negative to positive co-activates opioid and cannabinoid systems. Pain 2013;154:361–7. PubMed PMID: 23265686
Barron CJ, Moffett JA, Potter M. Patient expectations of physiotherapy: definitions, concepts, and theories. Physiother Theory Pract 2007;23:37e46. PubMed PMID: 17454797
Bialosky JE, Bishop MD, Cleland JA. Individual expectation: an overlooked, but pertinent, factor in the treatment of individuals experiencing musculoskeletal pain. Phys Ther 2010;90:1345e55. PubMed PMID: 20592270
Puentedura EJ, Cleland JA, Landers MR, Mintken PE, Louw A, Fernandez-de-Las-Penas C. Development of a clinical prediction rule to identify patients with neck pain likely to benefit from thrust joint manipulation to the cervical spine. J Orthop Sports Phys Ther 2012;42:577e92. PubMed PMID: 22585595
Colloca L, Benedetti F. How prior experience shapes placebo analgesia. Pain 2006;124:126e33. PubMed PMID: 16701952
O'Keeffe M, Cullinane P, Hurley J, Leahy I, Bunzli S, O'Sullivan PB, et al. What influences patient-therapist interactions in musculoskeletal physical therapy? Qualitative systematic review and meta-synthesis. Phys Ther 2015. PubMed PMID: 26427530
Petrie KJ, Rief W. Psychobiological mechanisms of placebo and nocebo effects: pathways to improve treatments and reduce side effects. Annu Rev Psychol 2019;70:1-27. PubMed PMID: 30110575
Stenberg G, Fjellman-Wiklund A, Ahlgren C. “Getting confirmation”: gender in expectations and experiences of healthcare for neck or back patients. J Rehabil Med 2012;44:163e71.
Hush JM, Cameron K, Mackey M. Patient satisfaction with musculoskeletal physical therapy care: a systematic review. Phys Ther 2011;91:25e36. PubMed PMID: 21071504
Lucassen P, Olesen F. Context as a drug: some consequences of placebo research for primary care. Scan J Prim Health Care 2016;34:428-33. PubMed PMID: 27978780
Sternberg E, Critchley S, Gallagher S, Raman VV. A self-fulfilling prophecy: linking belief to behavior. Ann N Y Acad Sci 2011;1234:83e97. PubMed PMID: 21988253
Gracely RH, Dubner R, Wolskee PJ, Deeter WR. Placebo and naloxone can alter post-surgical pain by separate mechanisms. Nature. 1983 Nov 17-23;306(5940):264-5. PubMed PMID: 6646208
Ferreira PH, Ferreira ML, Maher CG, et al. The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Phys Ther. 2013;93(4):470–478. PubMed PMID: 23139428
Schönberger M, Humle F, Teasdale TW. The development of the therapeutic working alliance, patients' awareness and their compliance during the process of brain injury rehabilitation. Brain Inj. 2006 Apr;20(4):445-54. PubMed PMID: 16716990
Burns JW, Evon D. Common and specific process factors in cardiac rehabilitation: independent and interactive effects of the working alliance and self-efficacy. Health Psychol. 2007 Nov;26(6):684-92. PubMed PMID: 18020839
Flückiger C, Del Re AC, Wampold BE, Horvath AO.The alliance in adult psychotherapy: A meta-analytic synthesis. Psychotherapy (Chic). 2018 Dec;55(4):316-340. PubMed PMID: 29792475
Brunner E, Dankaerts W, O‘Sullivan K, Meichtry A, Bauer C, Probst M. Associations between alliance, physiotherapists’ confidence in managing the patient and patient-reported distress in chronic low back pain practice. European Journal of Physiotherapy. 2019.
Colloca L. Placebo, nocebo, and learning mechanisms. Handb Exp Pharmacol 2014;225:17e35. PubMed PMID: 25304524
Branthwaite A, Cooper P. Analgesic effects of branding in treatment of headaches. Br Med J (Clin Res Ed). 1981 May 16; 282(6276): 1576–1578. PubMed PMID: 6786566
{kind=link}