If so, do you know how you are able to feel these feels? To notice these feelings you need the help of an important sense called interoception. The word interoception might not sound very sexy, but this sense isreally important. It has a huge influence on many areas of our lives like self-regulation, mental health and social connection1.
Recent perspectives have identified inputs that come from inside the body (i.e. interoceptive) as core elements in human well-being. Interoceptive perceptions can be defined as the sense of the physiological status of the entire body. They encompass a broad range of relevant biological functions that serve conscious and unconscious processes. Interoception is an interactive process of receiving, accessing, appraising and integrating inner bodily signals, which depends on past experiences and the current individual mindset. The growing interest in understanding interoception is due to its relationship to emotions and feelings in healthy and clinical populations. Altered interoceptive processes have been identified in a broad range of clinical conditions such as chronic pain, eating disorders, anxiety, depression, addictions, post-traumatic stress disorder, insomnia, and several others. Disrupted interoceptive processing is found to be fundamental to the perception, modulation and chronification of pain, on both cortical and behavioral levels2.
Interoception is about how your body feels.
The central component of the interoceptive system is the anterior insular cortex, which receives information through a vast network of small un-myelinated fibers. These fibers, called C-fibers, report a wide range of inputs such as: hunger, thirst, pain, itch, temperature, muscle contraction, hormonal and immune activity and cardiorespiratory function3. These inputs are processed in the interoceptive matrix that creates a meta-representation of the active processes in the body based on an explicit lateralization of the cortex. Specifically, the left and the right insula are usually coactive in the interoceptive system. Parasympathetic inputs are preferentially processed by the left insula while sympathetic ones are usually processed by the right one. Certain interoceptive stimuli (e.g., hunger, thirst, visceral sensations) are quite difficult to reproduce in a controlled manner. Easily reproducible interoceptive inputs, such as pain and temperature, are generally processed by the right insula due to their sympathetic high valence.
Interoceptive awareness (IA) can be divided in three sub-constructs: interoceptive accuracy (IAc), sensibility (IAs), and interoceptive confidence (IAconf). IAc assesses the participant’s ability to accurately perceive inner bodily sensations. Cardiac interoceptive accuracy measured by heartbeat counting has been the most commonly used measure of interoceptive accuracy in the literature.
According to recent developments, IAc deficits are identified across different chronic conditions. Patients suffering from fibromyalgia and multisomatoform chronic pain disorder perform less on the heart beat counting (HBC) task4. Cardiac interoception does not represent the only IA assessment domain. Three studies used a tension production task, which requires participants to estimate muscle tension4. Patients with chronic low back pain had a lower accuracy in their perception of muscle contraction, underestimating the levels of their own muscle tension5. As overall conclusion, patients suffering from chronic pain demonstrate an impaired ability in correctly detecting and processing internal bodily states.
It would be most important to understand which psychophysiological factors are supporting these interoceptive deficits, to comprehend if a diminished access to interoceptive information is due to interferences from the chronic condition (bottom-up inputs) or from psychological, emotional, and cognitive input (top-down input) that hinder the processing of these inner sensations.
How to improve interoception:
Mindfulness practices have been shown to be one of the most effective, evidence-based interventions for improving interoceptive awareness. Interestingly mindfulness is shown to activate the insula, the interoceptive center in the brain. That is why those who practice meditation often have superior levels of interoception. Activities such as yoga or mindfulness-based stress reduction are often cited as a second-line or adjunctive treatment option for chronic pain and are increasingly proposed by algologists or requested by patients.
There is increasing evidence that these approaches produce functional effects leading to an increase of body awareness and a decrease of pain through insular neuroplasticity. Taken together, significant elements support the association between body awareness, pain management and interceptive abilities5. Although interoceptive accuracy did not change after mindfulness training, an important increase in interoceptive sensibility was observed. When analyzed separately, five out of eight MAIA (Multidimensional Assessment of Interoceptive Awareness) - subscales had higher scores after the mindfulness training, whereas no change was observed in the active control group6. The greatest changes after attentional training were seen in self-regulation, representing the ability to regulate psychological distress by attention to bodily sensation. The second-largest increase after mindfulness training was seen in attention regulation, representing the ability to sustain and control attention to body sensations6.
The consequence of such mindfulness training practice is the deconditioning and eventual extinction of interoceptive appraisal habits, which can provide relief from catastrophization of interoceptive experience, a core feature of pain and anxiety disorders6. In this sense, it is plausible to suggest that attention regulation training based on a mindful attitude would lead to important changes in the attentional style of perceiving and interpreting body sensations.
The interoceptive system is also involved in innate analgesic mechanisms, which rely on specific stimulation of the peripheral C-Tactile (CT) afferent system. This system is composed of free tactile arborizations on the superficial layer of non-glabrous skin, forming a secondary touch system that is interoceptive rather than purely somatosensory. Parasympathetic interoceptive stimulation has been proven to modulate pain3.
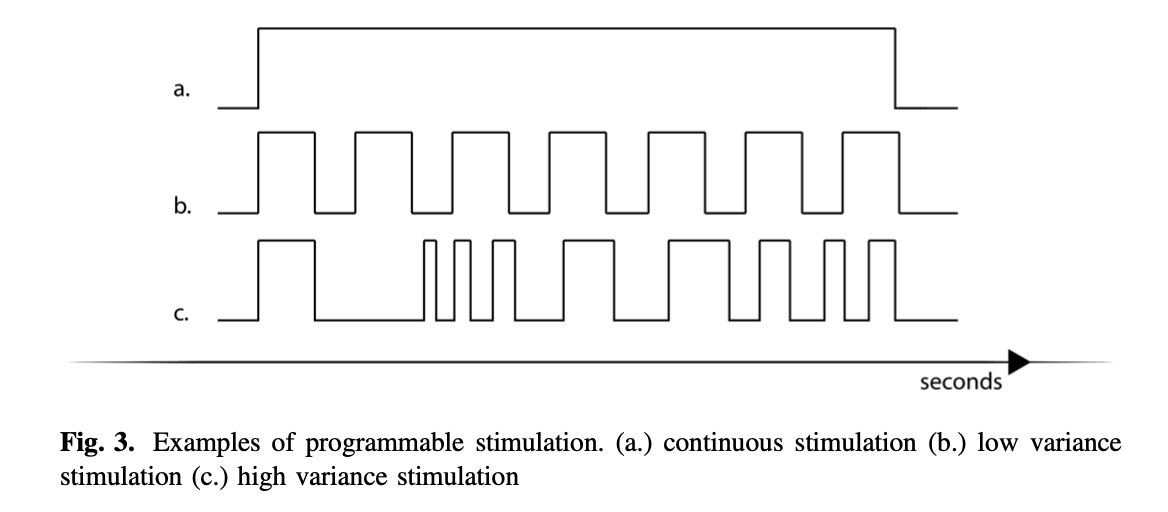
A new technological portable device is able to deliver such interoceptive parasympathetic stimuli and allows continuous stimulation to any chosen body site along with the ability to program variance and frequency of the delivered stimuli. Daniele Di Lernia et al. 2020 tested the device in a single-blind between-subjects design (N = 51) with primary, secondary musculoskeletal, and neuropathic chronic pain patients. The treatment specifically activates the CT system, by means of controlled stimulation of interoceptive unmyelinated afferents, at 3 cm/s with a force of 2.5mN. This treatment led to significant pain reduction in the chronic pain treatment group, while chronic pain controls who received comparable but non-interoceptive stimulation reported no change in pain intensity.
In conclusion, interoception should be envisaged as a target or an approach for future treatments in chronic pain conditions. This domain could offer innovative path of interventions, at the interface between the mind and the body5. Although pain is inherently interoceptive, interoceptive capabilities are still not adequately considered in the evaluation of patients with chronic pain in both treatment and research.
Luc Vanderweeën
Master of Science in Spinal Manual Therapy and Physiotherapy
Rug-Schouder-Nekcentrum, Schepdaal, Belgium
Pain in Motion International Research Group
2023 Pain in Motion
References and further reading:
1https://www.kelly-mahler.com/what-is-interoception...
2Altered Interoceptive Perception and the Effects of Interoceptive Analgesia in Musculoskeletal, Primary, and Neuropathic Chronic Pain Conditions. Di Lernia D, Lacerenza M, Ainley V, Riva G.J . Pers Med. 2020 Oct 29;10(4):201.
3Toward an Embodied Medicine: A Portable Device with Programmable Interoceptive Stimulation for Heart Rate Variability Enhancement. Di Lernia D, Cipresso P, Pedroli E, Riva . G.Sensors (Basel). 2018 Jul 30;18(8):2469.
4Pain in the body. Altered interoception in chronic pain conditions : A systematic review. Di Lernia D, Serino S, Riva G. Neurosci Biobehav Rev. 2016 Dec; 71:328-341.
5Interoception and social cognition in chronic low back pain: a common inference disturbance? An exploratory study. Florent El Grabli, François Quesque, Céline Borg, Michael Witthöft, George A Michael, et al. Pain Management Nursing, 2022, 12(4):471-485.
6The impact of a brief mindfulness training on interoception: A randomized controlled trial. Geissy Lainny de Lima-Araujo, Geovan Menezes de Sousa Júnior, Thatiane Mendes, Marcelo Demarzo, Norman Farb, Draulio Barros de Araujo, Maria Bernardete Cordeiro de Sousa. PLoS One, 2022, 17(9):e0273864.
{kind=link}